
Cranial and Sucking Complications from Hospitalization
Aug 21, 2025

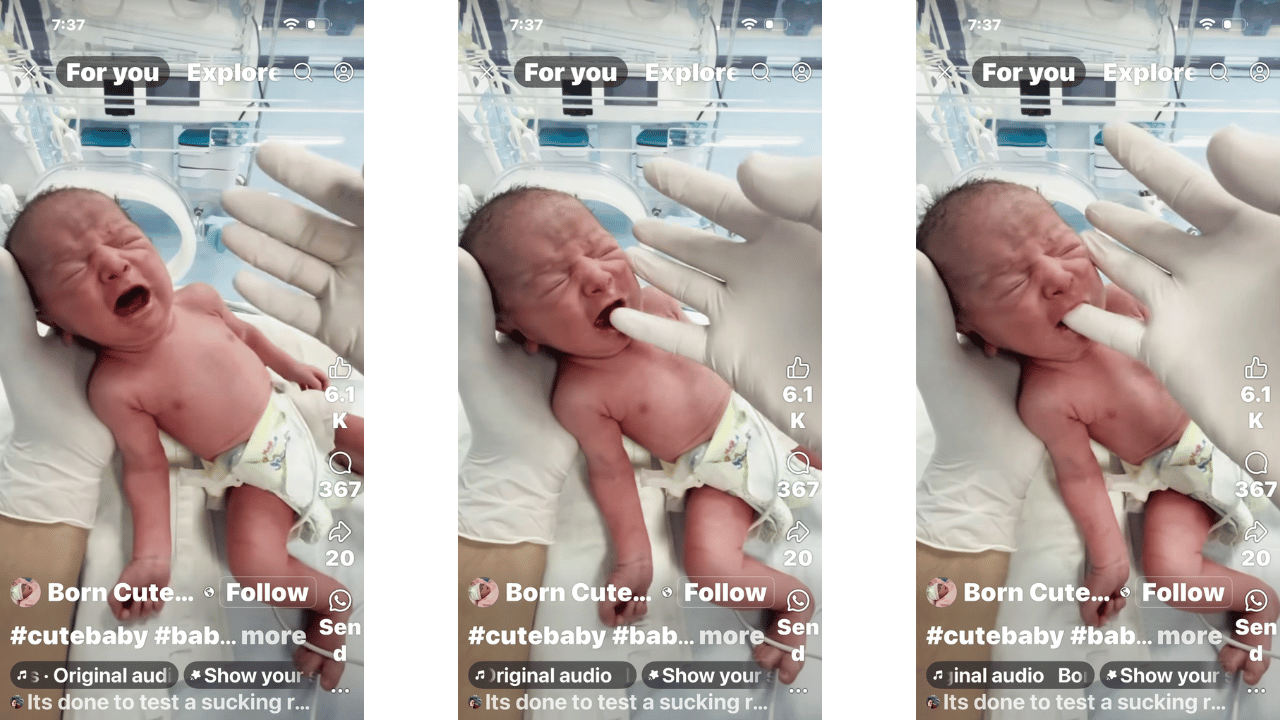
These stills show a premature infant undergoing what appears to be a suck reflex assessment in a NICU setting. Even in photos, valuable insight can be gathered about rotational initiation, tone distribution, visual tracking attempts, and overall system engagement.
Let’s break it down using observational movement markers:

 Neuromotor Engagement
Neuromotor Engagement
-
Facial Tension & Tone: The baby's expressions suggest a strong sympathetic response (crying, high tone in the face, furrowed brow), which is common when rotational input or sensory pressure is not integrated throughout the body—especially the occipital and cranial plates.
-
Suck Reflex Activation: In later frames, there's a visible oral rooting/suck response triggered by finger insertion. However, the neck remains hyperextended, indicating the suck is isolated—not yet integrated with spinal elongation or facial release. This often signals segmental delay.
 Rotational Axis & Rib Cage Movement
Rotational Axis & Rib Cage Movement
-
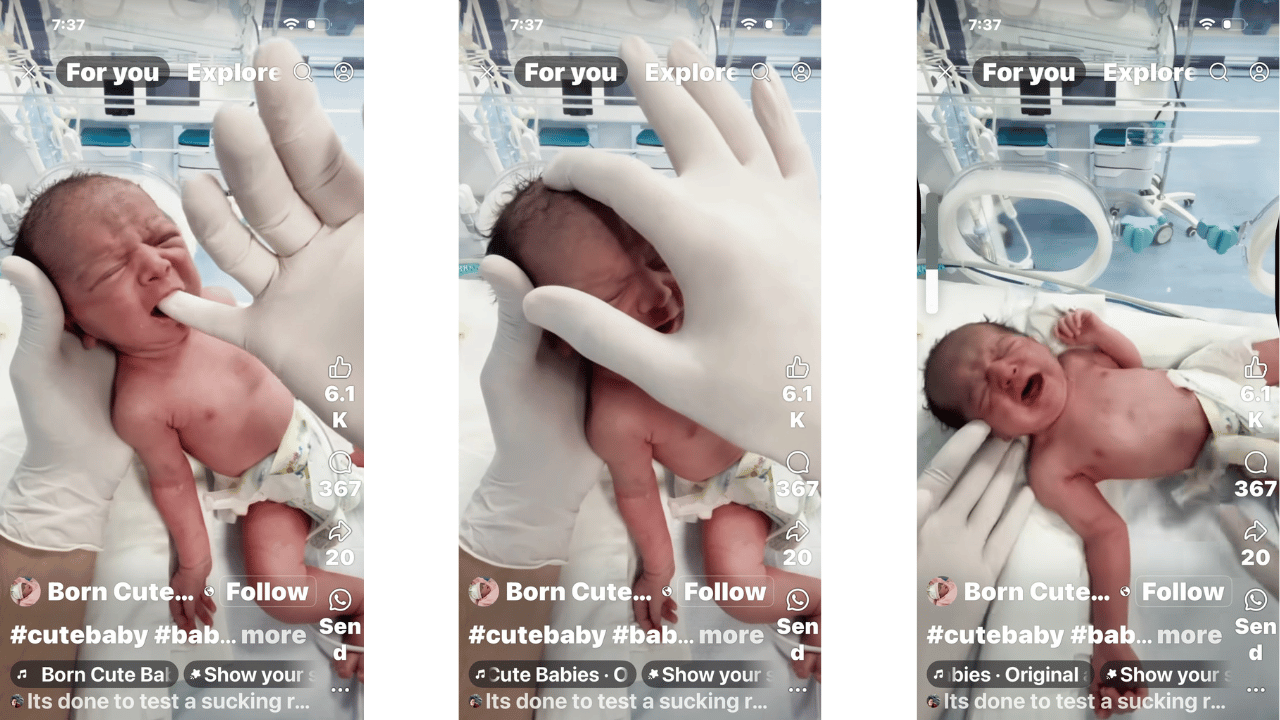
Lack of Rib Rotation: There’s no visible fluidity or expansion in the rib cage or torso—even when the arms move or when crying. Movement appears compressed and initiated only from distal effort (arms flailing, facial grimacing) rather than central core release, particularly from T7–T10.
-
Pelvic Lockdown: In most frames, the pelvis and legs are largely immobile or retract asymmetrically. The lower limbs show high tone in adduction but lack counter-rotation, pointing to delayed sacral activation. This can impair primitive reflex integration later.
 Postural Foundation & Weight Transfer
Postural Foundation & Weight Transfer
-
Shoulder Girdle Rigidity: While being held or touched, the baby shows little shoulder blade glide or axillary rotation. Instead, there is a collapsing inward toward the sternum, which can lead to early compensatory head-turning without spinal support (ATNR patterns that never resolve).
-
No Signs of Anti-Gravity Engagement: Even when "propped" in the clinician’s hand, there's minimal effort from the baby to lift or stabilize the trunk—suggesting underdeveloped transverse and sagittal plane transitions.
 Vision & Eye Engagement
Vision & Eye Engagement
-
No Peripheral Seeking: The baby's eyes do not appear to track or seek toward the clinician's face or finger. Instead, the gaze remains disconnected, which reflects a lack of spinal-visual link—vital for early orientation and later cognitive mapping.
 What This Child Needs Next
What This Child Needs Next
-
Rotational coaxing from occiput to sacrum using featherlight lifts and counterpressures
-
Work under the scapula and clavicle to introduce float—not press
-
Side-lying visual activation while allowing spinal extension
-
Gradual midline activation through inner thigh and heel counterbalances—not external arm support